

Abstract
This article investigated the relationship between age at onset of canonical babbling and audibility of amplified speech in children with hearing impairment. Thirteen children with severe–profound hearing impairment and two children with normal hearing participated in a longitudinal investigation of vocalization development. A nonconcurrent multiple baseline design was used to analyze vocalization recordings obtained during two phases (hearing aid [HA] and cochlear implant [CI]). Audibility during HA and CI use was calculated using the Speech Intelligibility Index (SII). Earlier ages of canonical babble onset were related to greater audibility of the speech signal during HA use. Children who developed canonical babble had an SII of .35 or greater. SII was a statistically significant predictor of age of onset of canonical babble. Results support the concept of an “essential” level of audibility for onset of canonical babble. Findings are discussed relative to their methodological and clinical implications regarding treatment decision making.
Universal newborn hearing screening has become a standard of care. As a result, the average age of identification of congenital hearing loss has declined. Approximately half of all infants identified with hearing impairment are now diagnosed by 3 months of age (Centers for Disease Control and Prevention, 2007), representing an improvement from the once typical age of 2.5 years (National Institutes of Health Consensus Statement, 1993; Vohr, Carty, Moore, & Letourneau, 1998). This decline has resulted in new challenges for parents of young children with hearing impairment and the professionals working with them, including making treatment decisions earlier than in the past. However, during the first year of life, limitations exist in the ability to assess degree and configuration of hearing loss (Gorga, Worthington, Reiland, Beauchaine, & Goldgar, 1985; Hicks, Tharpe, & Ashmead, 2000, Johnson & Brown, 2005; Vander Werff & Brown, 2005) and the ability of a hearing aid (HA) to provide benefit for an individual child (Hedley-Williams, Tharpe, & Bess, 1996; Seewald, Hudson, Gagne, & Zelisko, 1992; Seewald, Mills, Bagatto, Scollie, & Moodie, 2008; Seewald & Scollie, 2003; Stelmachowicz & Hoover, 2009).
Because of the urgency to make decisions regarding technology and to access the benefits of early intervention, the determination of HA benefit is especially crucial for parents of children with severe–profound hearing impairment who may benefit from a cochlear implant (CI). Benefit from amplification has traditionally been difficult to demonstrate in children too young to complete direct measures of speech and language abilities. Guidelines and methods to determine HA benefit in very young children are necessary to assist parents in their decision making. The study of infant vocalizations prior to first words may assist in establishing such guidelines and methods and subsequently aid in the selection of treatment options for severe–profound congenital hearing loss in young children.
Infant vocalizations are a particularly promising tool because of their robustness in children with normal hearing and their sensitivity to hearing impairment. The consensus is that canonical babble, a vocalization containing a minimum of a consonant and a vowel, is a precursor to first words and emerges in children with normal hearing between 7 and 10 months of age (Oller, 1980; Stark, 1980). Age of onset of canonical babble remains robust in children with normal hearing, even in the presence of certain risk indicators for developmental delay (Eilers et al., 1993; Lynch et al., 1995; Smith & Oller, 1981).
Differences in canonical babble between children with normal hearing and children with hearing impairment have been demonstrated. Children with milder degrees of hearing loss and greater audibility of the speech signal babble differently from those with more severe losses and less audibility of the speech signal (Moeller et al., 2007; Rvachew, Slawinski, Williams, & Green, 1999; Stoel-Gammon & Otomo, 1986). Studies investigating vocal development in infants with severe–profound hearing impairment found a substantial delay in the onset of canonical babble and a reduction in the volume of babble (Eilers & Oller, 1994; Ertmer & Mellon, 2001; Kent, Osberger, Netsell, & Goldschmidt Hustedde, 1987; Moeller et al., 2007; Oller & Eilers, 1988; Oller, Eilers, Bull, & Carney, 1985).
Oller et al. (Oller, 2000; Oller & Lynch, 1992; Steffens, Oller, Lynch, & Urbano, 1992) described in detail an approach to quantify canonical babble. This approach is termed the infraphonological approach. The remarkable components of the canonical syllable as defined by the infraphonological approach include (a) a single center (nucleus) with normal phonation and full resonance, (b) at least one margin (consonant-like sound) resulting from movement of the vocal tract, and (c) a rapid uninterrupted transition from margin to nucleus (Oller, 2000). In addition, a canonical syllable ratio (CSR) of at least 0.15 must be achieved to indicate that a child has entered the canonical babbling stage. A CSR is calculated by counting the number of canonical syllables and dividing by the total number of syllables, excluding vegetative (reflexive) vocalizations. In calculating the CSR, the identification of canonical syllables is traditionally conducted auditorily/perceptually (D. K. Oller, personal communication, November, 8, 2007). The rationale for the auditory identification of canonical syllables relates to the difficulty in defining acoustic parameters and more specifically, in measuring formant transitions. In addition, research supports the ability of listeners to perceptually identify the canonical syllable. For example, Oller, Eilers, and Basinger (2001) reported on a series of studies that investigated the ability of parents to accurately identify onset of canonical babbling. They concluded that with little to no training, parents were able to predict the onset of canonical babbling.
A limitation of using vocal development in young children as a decision variable for cochlear implantation is the failure to adequately address the issue of speech audibility provided by the HA fitting. If the HA is not fit properly, then a decision to place a CI may be premature. Limitations exist in our ability to assess HA benefit. For infants and toddlers, parent report of auditory skill development and early speech development are the primary tools used to gauge the degree of benefit from HA use (Kishon-Rabin, Taitelbaum-Swead, Ezrati-Vinacour, & Hildesheimer, 2005; Robbins, Koch, Osberger, Zimmerman-Phillips, & Kishon-Rabin, 2004). Although parent report provides important information, a case is made for the inclusion of direct observation and play-based measures to provide a more thorough depiction of a child’s development (Nikolopoulos, Archbold, & Gregory, 2005; Pinto, Lacerda, & Porto, 2008). Other measures used to gauge HA benefit, such as aided audiograms, have been shown to inaccurately reflect the benefit of nonlinear HAs (Seewald et al., 1992). Seewald et al. found that, in many cases, the aided audiogram overestimated the sensation level of amplified speech and that probe microphone measures allowed for a more accurate depiction of the sensation level of amplified speech.
Numerous audiological practice guidelines stress the need for a systematic approach to the fitting of HAs that takes into account the acoustic characteristics of the child's ear with probe microphone measures and maximizes the audibility of speech within a safe and comfortable range (American Academy of Audiology, 2004; Ministry of Children and Youth Services, 2007; The Pediatric Working Group, 1996). Yet, not all practitioners employ the use of probe microphone measures in the fitting of HAs in the pediatric population (Hedley-Williams et al., 1996; Rigsby, Bradham, Dickinson, & Mueller, 2007; Seewald et al., 2008).
Although systematic procedures are not yet consistently used to assess the fitting of HAs and to ensure audibility, research supports that audibility is important to early infant vocal production (Eilers & Oller, 1994; Ertmer & Mellon, 2001; Moeller et al., 2007; Stoel-Gammon & Otomo, 1986). Stoel-Gammon and Otomo and Moeller et al. reported that infants with milder degrees of hearing loss (and presumably more audibility of the speech signal) displayed fewer differences in canonical babble from children with normal hearing than did children with more significant losses. Ertmer and Mellon detailed a case study in which a child displayed little benefit from HA use as evidenced by a lack of vocal development. Once provided with a CI, this child progressed more rapidly in her vocal development than would be expected for a child with normal hearing. This increase in vocal development was primarily attributed to the increased audibility received from the CI.
Two final studies of note regarding the relationship between audibility and vocal development include Hapsburg and Davis (2006) and Eilers and Oller (1994). Hapsburg and Davis examined the relationship between auditory sensitivity and vocalization patterns in 15 infants with hearing sensitivity ranging from normal hearing to profound hearing impairment. They identified a significant relationship (R2 = 0.53) between the unaided pure-tone average and the percentage of utterances containing canonical syllables. Eilers and Oller found that age of amplification moderately correlated (0.68) with age of onset of canonical babble. Findings from this study suggested that the younger a child received amplification (and presumably additional audibility), the younger he began canonical babble. A limitation of Hapsburg and Davis, and Eilers and Oller as well as other research linking audibility with canonical babble/speech outcomes is a consistent lack of information regarding adequacy of the HA fitting. Rarely is information beyond a pure-tone average and age of amplification provided.
In summary, audibility of the speech signal is apparently important to infant vocal production and is associated with better speech outcomes, yet as most recently demonstrated by Rigsby et al. (2007), practice variation exists in the fitting of HAs in the pediatric population. Furthermore, studies of vocal development in infants with hearing impairment reported limited, if any, information regarding the HA fitting. The purpose of this article was to investigate the relationship between age at onset of canonical babbling and audibility of speech in infants and toddlers during HA and CI use. This article attempted to fill a gap in the literature by examining the onset of canonical babble in conjunction with audibility measures. A secondary purpose was to compare the age at onset of canonical babbling as determined using the standard CSR measure and an examiner created canonical babble utterance ratio (CBUR) measure.
In this article, it was hypothesized that age of onset of canonical babble would decrease as audibility of the speech signal increased. In addition, it was expected that an essential level of audibility would be necessary for a child to enter the canonical babbling stage. These hypotheses were tested by examining the relationship between canonical babble and audibility of speech, and patterns of vocal development in young children with severe–profound hearing impairment.
Method
Participants
Children with hearing impairment.
Thirteen children (six males and seven females) with hearing impairment from various cities in Iowa participated in this study. The children began the longitudinal study at an average age of 13.6 months (range 4.5–19 months) and completed the study at an average age of 31.8 months (range 25–37.5 months). Initially, all participants with hearing impairment were HA users. Seven of the children were fit with HAs by 12 months of age and six were fit with HAs by 18 months of age. All participants with hearing impairment were considered potential CI candidates based on their poorer ear pure-tone averages (PTAs). All participants received a CI during the course of this study at an average age of 17 months (range 12–23 months). Better ear PTAs (average of thresholds at 500, 1000, and 2000 Hz) based on behavioral audiological evaluation and physiological testing ranged from 68 dBHL to no response at the limits of the audiometer. All children’s cognitive abilities appeared to be “within normal limits” in accordance with the Bayley scales of infant development—II’s “Mental” subscale.13 (Bayley, 1993). All children had no known visual abnormalities or motor delays. American English was the language spoken in each child’s home. In addition, all children utilized a system of total communication in the home that involved the use of sign language in American English word order. See Table 1 for demographic information on individual study participants.
Table 1.
Demographic information of participants with hearing impairment
| Participant | Etiology of hearing loss | UNHS | Age identified (months) | Age fit with HAs (months) | Age enrolled (months) | Better ear PTA (500, 1000, and 2000 Hz) (dBHL) | Length of HA use (months) | Length of CI (months) |
| Axel | Unknown | No | 9 (OM) | 17 | 18.5 | 110 | 3.5 | 12 |
| Norman | Unknown | Yes | 4 (OM) | 5.5 | 14.7 | 68 | 14 | 12 |
| Jane | Cochlear malformation (Mondini) | Yes | 9.7 | 10 | 11 | 93 | 8 | 12 |
| Levi | Hereditary (not specified) | Yes | Unknown | 5 | 5 | 87 | 9.75 | 12 |
| Cathy | Unknown | Yes | 4 | 17 | 17 | 93 | 6.5 | 12 |
| Kyra | Unknown | Yes | 3.6 | 8 | 4.5 | No response | 15.25 | 12 |
| Sandra | Hereditary (Connexin 26) | Yes | 11.7 | 12 | 13 | 110 | 3 | 12 |
| Ben | CMV | Yes | 3 | 7 | 5 | No response | 6.75 | 12 |
| Mary | Unknown | No | 7.5 | 11 | 17 | 100 | 7 | 12 |
| Karl | Unknown | Unknown | 15 (OM) | 18 | 17 | 110 | 1.75 | 14 |
| Robert | Otoxicity | Unknown | 10 | 16.5 | 17 | 110 | 2 | 12 |
| Sheila | Hereditary (Connexin 26) | Yes | Unknown | 16 | 18 | 110 | 2.5 | 18 |
| Carrie | Unknown | Unknown | 13 (OM) | 17 | 19 | 100 | 1.5 | 12 |
Notes. Participant names are pseudo-names. CI = cochlear implant; CMV = cytomegalovirus; HA = hearing aid; OM = history otitis media prior to diagnosis; PTA = pure-tone average; UNHS = universal newborn hearing screen.
Children with normal hearing.
Two children with normal hearing thresholds (both males) participated in this study. These children were selected from a group of normal hearing children being followed as part of a larger project. They were selected for inclusion in this study because they were the first two to reach 12 months of age by the end of data collection. The children began the study at 3 and 5 months of age and completed the study at 12 months of age. The children’s cognitive abilities appeared to be “within normal limits” in accordance with the Bayley scales of infant development—II’s “Mental” subscale.13 (Bayley, 1993). Neither had known visual abnormalities or motor delays. American English was the language spoken in each child’s home.
Data from these normal hearing children were included in the current study to illustrate that the data collection and analysis procedures were able to capture the emergence of canonical babble in the time frame indicated in the literature for children with normal hearing. These children were not intended to serve as a control group, yet they do represent one end of the continuum of audibility.
Design
A nonconcurrent multiple baseline design (Kennedy, 2005) was used to analyze recordings obtained during two phases (A = HA and B = CI). Recordings during the A phase were obtained and analyzed while the participants received other forms of assistive technology (e.g., HAs). Data for this phase were collected prior to a participant’s receiving his/her CI. Recordings during the second phase were obtained and analyzed following stimulation of the CI for each participant.
Procedures
Caregivers were asked to return on a monthly basis for a vocalization recording to be obtained with a digital audio tape recorder (Sony, TCD-D100, Japan) and for the session to be videotaped. Every attempt was made to coordinate vocal recordings with scheduled visits to the University for audiological and/or HA evaluations. At each visit, an elicited and spontaneous vocalization sample was collected in a quiet therapy room. Collection of the elicited and spontaneous vocalization samples was achieved in the same session with little to no interruption. The spontaneous sample was obtained by enriching the child’s environment with age-appropriate toys and allowing the child’s caregiver(s) to engage in play activity with their child. The elicited vocalization sample was obtained through interaction with the examiner. The length of each session varied between 15 and 30 min, with an occasional session lasting longer depending on the status of the child and the willingness of the family.
Two home visits were made to two separate families to collect vocalization data. The same protocol and toys were used for both visits. These home visits were conducted to prevent disruption of the data collection schedule.
Data Analysis
Vocalization coding.
Digital audio tape recordings from each participant’s sessions were coded using the !OBSERVE data collection software (Sander, 2001). The software allowed the user to assign keys of the computer keyboard to vocalization types of interest. During coding, a key was pressed that corresponded to the vocalization type heard. A second-by-second record of coding and a frequency count of each vocalization type were generated. Vocalizations were coded into one of the three types: (a) Canonical, (b) Word, and (c) Other. Vocalization types were based on the stages of infant vocal development of Oller (1980) and Stark (1980) and were coded once per breath group during a first pass of coding. A breath group was defined as a vocalization or grouping of vocalizations demarcated by a period of quiet of at least 2 s. Definitions used to code vocalization type as well as coding rules for use during the first pass of coding are included in the Appendix A.
A second pass of coding was conducted in order to determine the number of syllables produced during each session. A CSR was calculated for each session of each participant until the criterion of a CSR of at least 0.15 was established. A CSR was calculated by counting the number of canonical syllables in a session and dividing by the total number of syllables in that session (Oller, 2000; Oller & Lynch, 1992; Steffens et al., 1992). See Appendix B for detailed instructions for conducting the syllable count.
A second ratio, the CBUR, was calculated for all sessions of each participant. The CBUR was defined by this investigator as the number of canonical utterances (at the level of the breath group) divided by the total number of utterances (at the level of the breath group). The CBUR is a ratio to compare the quantity of canonical utterances with the child's overall utterance production.
Using independent trained listeners, interobserver agreement was obtained for 30% of each participant's sessions during the HA phase as well as 30% of each participant's sessions during the CI phase. For the participants with normal hearing, interobserver agreement was obtained for 30% of each participant's sessions. Agreement was calculated separately for each vocalization type. Agreement sessions were randomly selected for each participant. An agreement was defined as the same type and number of vocalization scored by both listeners within ±3 s of each other. A disagreement was defined as one listener scoring a vocalization that the other listener either did not score or disagreed regarding type or number. Agreement percentages were calculated based on 6-s interval-by-interval comparisons of the listeners’ records, in which the smaller number of responses in each interval was divided by the larger number of responses. These fractions were then summed across all intervals, divided by the total number of intervals in the session, and multiplied by 100 to obtain the percent agreement between the two listeners. See Table 2 for mean agreement scores and ranges for each participant.
Table 2.
Mean interobserver agreement (IOA) scores and ranges for each participant
| Participant information |
Other |
Canonical |
Word |
||||
| Name | Phase | Mean % | Range % | Mean % | Range % | Mean % | Range % |
| Axel | HA | 93 | 90–97 | 99 | 98–100 | 100 | — |
| CI | 93 | 83–100 | 97 | 92–100 | 100 | — | |
| Norman | HA | 86 | 78–90 | 92 | 90–96 | 100 | — |
| CI | 87 | 76–100 | 89 | 82–100 | 96 | 85–100 | |
| Jane | HA | 95 | 86–100 | 98 | 96–100 | 100 | — |
| CI | 93 | 90–96 | 96 | 94–98 | 99.4 | 98–100 | |
| Levi | HA | 93 | 91–96 | 98 | 91–100 | 100 | — |
| CI | 96 | 93–100 | 95 | 87–100 | 99 | 96–100 | |
| Cathy | HA | 90 | 84–97 | 100 | — | 100 | — |
| CI | 90 | 84–100 | 97 | 91–100 | 99.7 | 98–100 | |
| Kyra | HA | 97 | 90–100 | 100 | — | 100 | — |
| CI | 96 | 93–100 | 97 | 93–100 | 100 | — | |
| Sandra | HA | 98 | 95–100 | 100 | — | 100 | — |
| CI | 97 | 92–100 | 96 | 84–100 | 97 | 84–100 | |
| Ben | HA | 97 | 95–100 | 100 | — | 100 | — |
| CI | 95 | 86–100 | 99.7 | 97–100 | 99.9 | 99–100 | |
| Mary | HA | 97 | — | 100 | — | 100 | — |
| CI | 90 | 86–98 | 95 | 90–100 | 99.6 | 97–100 | |
| Karl | HA | 96 | 93–98 | 100 | — | 100 | — |
| CI | 81 | 76–86 | 89 | 87–91 | 100 | — | |
| Robert | HA | 99 | — | 100 | — | 100 | — |
| CI | 98 | 97–99 | 98 | 95–100 | 99.7 | 99–100 | |
| Sheila | HA | 100 | — | 100 | — | 100 | — |
| CI | 95 | — | 93 | — | 98.5 | 97–100 | |
| Carrie | HA | 86 | — | 100 | — | 100 | — |
| CI | 82 | 77–87 | 89 | 82–97 | 97 | 93–100 | |
| Mark | NH | 90 | 72–96 | 99 | 97–100 | 100 | — |
| Larry | NH | 95 | 82–100 | 99 | 93–100 | 100 | — |
Notes. A dash (—) indicates that no range exists (e.g., only one session was scored for agreement or the mean agreement was the same in all sessions scored). CI = cochlear implant; HA = hearing aid; NH = normal hearing.
An independent observer also redetermined the session/date of entry of each child into the canonical babbling stage. The observer did this by returning to the raw data and independently recounting syllables and recalculating the CSR for each session until the criterion (CSR = 0.15) for entry into the canonical babbling stage was met. For all 15 participants, there was 100% agreement regarding the date of entry into the canonical babbling stage.
Audibility.
In order to quantify audibility of speech for each child, the Speech Intelligibility Index (SII) was calculated. An SII is based on the ANSI S3.5-1997 and is highly correlated with the intelligibility of speech under a variety of adverse listening conditions. The SII is a measure designed to quantify the proportion of the speech signal that is audible to the listener, with enhanced weighting for the frequency regions of speech that carry the most information. The SII ranges from 0.0 to 1.0. An SII of 0.0 is consistent with none of the speech signal being audible, whereas an SII of 1.0 is consistent with normal hearing. In order to calculate an SII, the following information is required: (a) long-term average speech spectrum, (b) insertion gain for speech, and (c) thresholds in dBHL. Extrapolation and interpolation are used if necessary information is excluded.
In this article, the 1/3 octave band levels of the “hip position” from the SHARP program (Omaha, NE) (Stelmachowicz, Lewis, Kalberer, & Creutz, 1994) were used to calculate SII. All calculations of SII were based on the standard band importance function for standard speech. The hip position from the SHARP program was used to gain a more complete understanding of the audibility provided by a young child’s HAs in a typical listening situation (i.e., while being carried by the caregiver).
Insertion gain was also required in order to calculate SII. Insertion gain in 1/3 octave bands was calculated by taking each child’s measured real ear–aided response (REAR) and subtracting a norm-based real ear–unaided response (REUR) as well as the input level of the signal used to obtain an REAR. Real-ear measures for each child were obtained from the University’s Hearing Aid Center as well as from local providers, when available. The Hearing Aid Center verified HA fit using real-ear measures and the Desired Sensation Level fitting strategy (Moodie, Seewald, & Sinclair, 1994; Seewald, 1995). The Hearing Aid Center used a 65 dBSPL pure-tone sweep as the input signal to obtain REAR. REUR for calculation of the SII was obtained by using the age norms established by Kruger (1987) for infants and young children. In summary, the following equation was used to obtain insertion gain in 1/3 octave bands:
where IG = insertion gain, Xn = frequency of interest, REAR = real ear–aided response, REUR = real ear–unaided response, and IS = input signal.
The last requirement for calculation of SII was unaided threshold information. Unaided threshold information was obtained from chart review. The best most recent audiometric data were used for calculation of SII during HA use. See Table 3 for the SIIs calculated for each child during HA use. SII was calculated during CI use by inserting sound field behavioral thresholds, obtained with the child wearing the implant, in place of unaided threshold information. SII was calculated for the same speech spectrum as mentioned above. Insertion gain was not entered for the CI users. See Table 3 for the SIIs calculated for each child during CI use.
Table 3.
Speech Intelligibility Index (SII) by device
| Participant | Hearing aid, right ear | Hearing aid, left ear | Cochlear implant |
| Axel | .35 | .49 | .85 |
| Norman | .41 | .49 | .87 |
| Jane | .37 | .42 | .65 |
| Levi | .37 | .23 | .82 |
| Cathy | .16 | .35 | .69 |
| Kyra | .31 | .29 | .75 |
| Sandra | .26 | .25 | .87 |
| Ben | .23 | .09 | .93 |
| Mary | — | .17 | .79 |
| Karl | .13 | — | .74 |
| Robert | — | 0 | .72 |
| Sheilaa | .89 | ||
| Carriea | .78 | ||
| Mark | Normal hearing | Normal hearing | Not applicable |
| 1.0 | 1.0 | ||
| Larry | Normal hearing | Normal hearing | Not applicable |
| 1.0 | 1.0 |
Notes. SII can range from 0 (no audibility) to 1.0 (complete audibility). Bold type indicates SII of the best aided ear. A dash (—) indicates no data collected.
Data required for SII calculation, during hearing aid use, not on file.
Results
Age at Onset of Canonical Babbling and Audibility
It was predicted that age of onset of canonical babble would decrease as audibility of the speech signal increased. Figure 1 shows the relationship between chronological age of onset of canonical babbling and audibility (SII) for 13 participants. Two study participants were not included because detailed HA information was unavailable, and therefore, audibility (SII) could not be calculated. Chronological age of onset of canonical babbling represents the earliest age at which a vocalization recording with the criterion CSR of 0.15 for entry into the canonical babbling stage was obtained. Each data point represents one participant. Children with hearing impairment are represented by circles and children with normal hearing are represented by triangles. SIIs for the children with hearing impairment represent the best obtained during HA use. Greater SIIs are related to earlier chronological ages of onset of canonical babble. SII and chronological age of onset are related with an R2 = 0.54 (r = −.74, p = .0025). These results support the hypothesis that the more audible the speech signal (the greater the SII), the earlier the chronological age of onset of canonical babble.
Figure 1.

Relationship of chronological age of onset of canonical babble and hearing aid audibility (Speech Intelligibility Index [SII]).
Canonical Babble and Essential Audibility
It was also predicted that an essential level of audibility would be necessary for a child to enter the canonical babbling stage. Figure 2 displays the audibility (SII) during HA and CI use for 11 participants with hearing impairment. Two study participants were not included because detailed HA information was unavailable. SII during HA use represents audibility from the best hearing-aided ear. SII values during HA and CI use are displayed at the top of each of their respective bars on Figure 2. CSR values at onset of canonical babble are displayed in bold and vertically on the bars. Five participants (Axel, Norman, Jane, Levi, and Cathy) met criterion for onset of canonical babble during HA use with a CSR of ≥0.15. The remaining six participants with hearing impairment failed to meet criterion for onset of canonical babbling during HA use. Children who developed canonical babble during HA use had an SII of .35 or greater in the best hearing-aided ear. Children who failed to develop canonical babble during HA use had an SII of .31 or less in the best hearing-aided ear. It should be noted that all six participants who did not begin canonical babble during HA use began canonical babble during CI use when SIIs well exceeded those present during HA use. These data support the second hypothesis regarding the need for an essential level of audibility to facilitate the development of canonical babble during HA use. No children met criterion (CSR = 0.15) for entry into the canonical babble stage during HA use, with an SII of less than .35. Children who failed to develop canonical babble during HA use had an SII of .31 or less (in the best hearing-aided ear).
Figure 2.

Participant audibility (Speech Intelligibility Index [SII]) and canonical syllable ratio (CSR) by device. The x-axis represents each participant with hearing impairment during hearing aid (HA) use and during cochlear implant (CI) use. The y-axis represents the SII achieved with each device. The SII during HA use is represented by an open bar. The SII during CI use is represented by a shaded bar. The horizontal line at an SII = .35 represents an “essential” level of audibility. Participants whose SII during HA use met or exceeded .35 began canonical babble while wearing HAs (at a CSR = 0.15). The value of CSR at onset is indicated for each participant. CSR is shown in the open bar when onset occurred during HA use. CSR is shown in the shaded bar when onset occurred during CI use.
CBUR and CSR
To determine the utility of using the CBUR to identify entry into the canonical babbling stage, the two ratios were compared. Recall that the CBUR is a ratio of the number of canonical utterances divided by the total number of utterances and the CSR is a ratio of the number of canonical syllables divided by the total number of syllables. For all 15 participants, the CBUR was calculated for each session until termination of the study; the CSR was calculated for each session of each participant until he/she met criterion for entry into the canonical babbling stage (CSR ≥ 0.15).
For 14 of the 15 participants, it was found that a CBUR could be calculated for each session of each participant that accurately predicted entry into the canonical babble stage (CSR ≥ 0.15) at the same criterion (CBUR ≥ 0.15). There was one exception (to be discussed in the next section) in which CBUR and CSR disagreed regarding entry into the canonical babbling stage at a criterion of 0.15. For one participant (Axel) in whom this trend was not found, CSR predicted entry at 3.5 months hearing age, whereas CBUR predicted entry later at 8.6 months hearing age. It should be noted that Axel’s CBUR at 3.5 months hearing age was 0.14. See Table 4 for a summary of these results.
Table 4.
Age of onset of canonical babble
| Participant | Chronological age of onset (months) | Hearing age of onset (months) | CBUR predicted onset at same age (yes/no) |
| Axel | 20.5 | 3.5 (CSR); 8.6 (CBUR) | No |
| Norman | 14.75 | 9 | Yes |
| Jane | 11 | 1 | Yes |
| Levi | 12 | 7 | Yes |
| Cathy | 23 | 6.5 | Yes |
| Kyra | 33 | 12 | Yes |
| Sandra | 19 | 3 | Yes |
| Ben | 19.5 | 6 | Yes |
| Mary | 23.75 | 4.75 | Yes |
| Karl | 34.5 | 13.25 | Yes |
| Robert | 27.75 | 8 | Yes |
| Sheila | 24 | 4.5 | Yes |
| Carrie | 32 | 12.75 | Yes |
| Mark | 8 | 8 | Yes |
| Larry | 9 | 9 | Yes |
Notes. Age of onset represents when a child met the criterion of a CSR ≥ 0.15. At onset, the CBUR was also ≥ 0.15 with one exception (Axel). Axel’s age of onset for CBUR is indicated. CSR = canonical syllable ratio; CBUR = canonical babble utterance ratio.
Trends in Vocal Development
Individual participant data were included to highlight the finding that an essential level of audibility (for these data, SII ≥ .35) was necessary for the development of canonical babble. As such, figures were grouped according to audibility pre- and post-CI. Individual data should be examined for the emergence of canonical babble indicated by a CBUR of ≥0.15. Age at which emergence occurred is shown by a shaded bar on each figure.
Individual participant data were also included to portray the change in each child's vocal repertoire as hearing age increased. It should be noted that pseudo-participant names are provided on the figures for ease of reference.
Participant age.
Chronological age was calculated for each child for each session and represented the child's actual age in months. All participants were born within 1 month of their due dates and, therefore, chronological age represented the child's age from date of birth. Hearing age was also calculated for each child for each session and represented (a) the difference in months between the date the child was fit with HAs and the session date, provided that best ear-aided audibility was equivalent to an SII of at least .35 with the “hip” spectrum or (b) if best ear-aided audibility was less than 0.35 with the “hip” spectrum, hearing age represented the difference in months between the date the child's CI was stimulated and the session date. An SII criterion of .35 for hearing age onset during HA use was chosen because after the data were examined (Figure 2), this value represented the cutoff between children who failed to develop canonical babble during HA use and children who developed canonical babble while wearing HAs.
Individual data: children with hearing impairment.
Two patterns of vocal development were observed for the participants with hearing impairment. In general, the first pattern consisted of the emergence of canonical babble during HA use with SIIs ≥.35. Five participants fit this pattern. The results of Pattern 1 are displayed in Figures 3 and 4. Axel, Norman, and Cathy (Figure 3) began canonical babble at 3.5, 9.0, and 6.5 months hearing age, respectively. Levi and Jane (Figure 4) began canonical babble at 7.0 and 1.0 months hearing age, respectively. Four of the five children with this pattern of vocalization development began first oral-word production during the course of this study. First oral words for these four children were documented at an average chronological age of 24.5 months (range 22–30.25 months). Finally, it should be noted that once children achieved a CBUR of ≥0.15, subsequent CBURs generally did not fall below this value.
Figure 3.
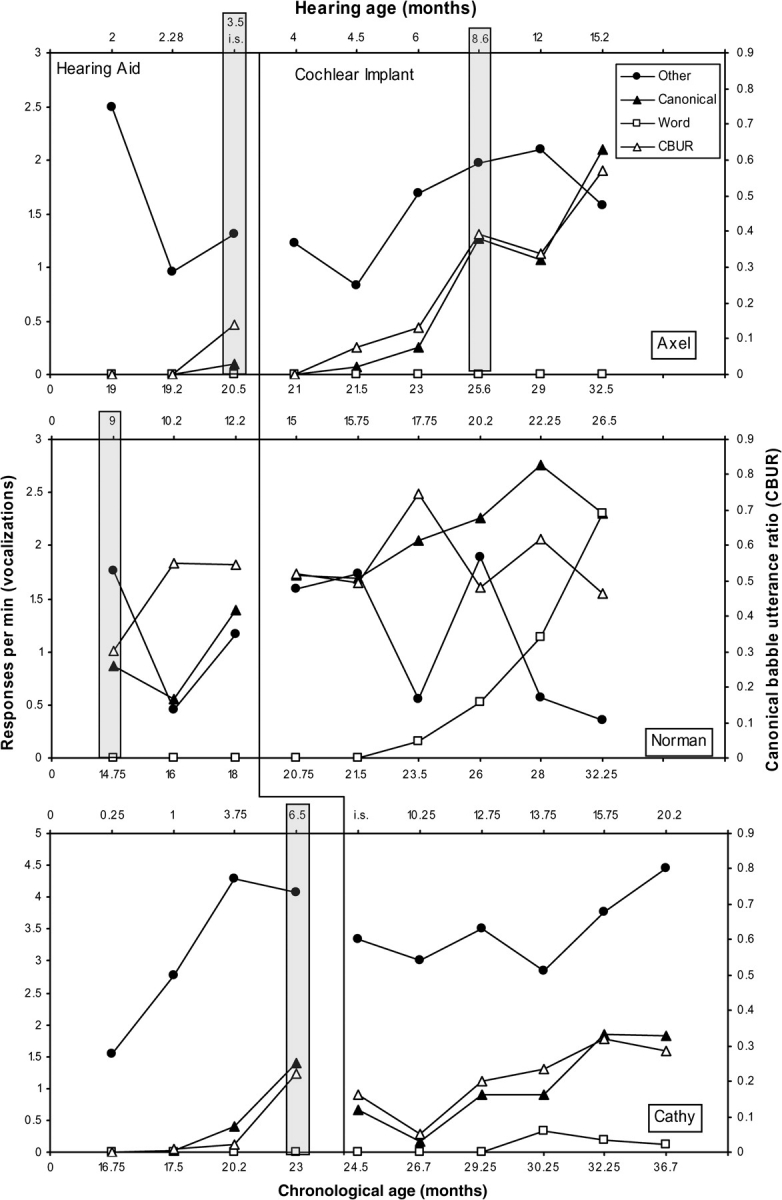
Responses per minute of vocalizations for participants with hearing impairment who met criterion for audibility during hearing aid (HA) use (Speech Intelligibility Index ≥ .35), Axel (top), Norman (center), and Cathy (bottom). The lower x-axis represents the child's chronological age in months, and the upper x-axis represents the child's hearing age in months. I.S. indicates the day of initial stimulation of the cochlear implant (CI). An i.s. within the HA phase indicates that the vocalization sample was obtained on the day of initial stimulation but prior to initial stimulation. An i.s. within the CI phase indicates that the vocalization sample was obtained on the day of initial stimulation following initial stimulation. The absence of an i.s. indicates that no vocalization sample was obtained on the day of initial stimulation. The left y-axis represents the child's responses per minute of each of the three vocalization types as a function of age. The right y-axis represents the child's canonical babble utterance ratio (CBUR). The shaded vertical bar indicates the age of emergence of canonical babble at a criterion canonical syllable ratio (CSR) and CBUR ≥ 0.15. For Axel, the bar during the HA phase indicates when the criterion CSR was met and the bar during the CI phase indicates when the criterion CBUR was met. For all other participants, criterion for both CSR and CBUR were met at the same age.
Figure 4.

Responses per minute of vocalizations for participants with hearing loss who met criterion for audibility during hearing aid (HA) use (Speech Intelligibility Index ≥ .35), Levi (top) and Jane (bottom). The lower x-axis represents the child's chronological age in months, and the upper x-axis represents the child's hearing age in months. I.S. indicates the day of initial stimulation of the cochlear implant (CI). An i.s. within the HA phase indicates that the vocalization sample was obtained on the day of initial stimulation but prior to initial stimulation. An i.s. within the CI phase indicates that the vocalization sample was obtained on the day of initial stimulation following initial stimulation. The left y-axis represents the child's responses per minute of each of the three vocalization types as a function of age. The right y-axis represents the child's canonical babble utterance ratio (CBUR). The shaded vertical bar indicates the age of emergence of canonical babble at a criterion canonical syllable ratio and CBUR ≥ 0.15.
In general, the second pattern consisted of the emergence of canonical babble during CI use. These participants’ SIIs were ≤0.31 during HA use and did not exceed .31 until after cochlear implantation. The results of Pattern 2 are displayed in Figures 5–7. Carrie, Sheila, and Robert (Figure 5) began canonical babble at 12.75, 4.5, and 8 months hearing age, respectively. Mary, Sandra, and Karl (Figure 6) began canonical babble at 4.75, 3, and 13.25 months hearing age, respectively. Ben and Kyra (Figure 7) began canonical babble at 6 and 12 months hearing age, respectively. Five of the eight children with this pattern of vocalization development began first oral-word production during the course of this study. First oral words for these five children were documented at an average chronological age of 27.9 months (range 21.75–37.5 months). Finally, it should be noted once children achieved a CBUR of ≥0.15, subsequent CBURs did not fall below this value.
Figure 5.
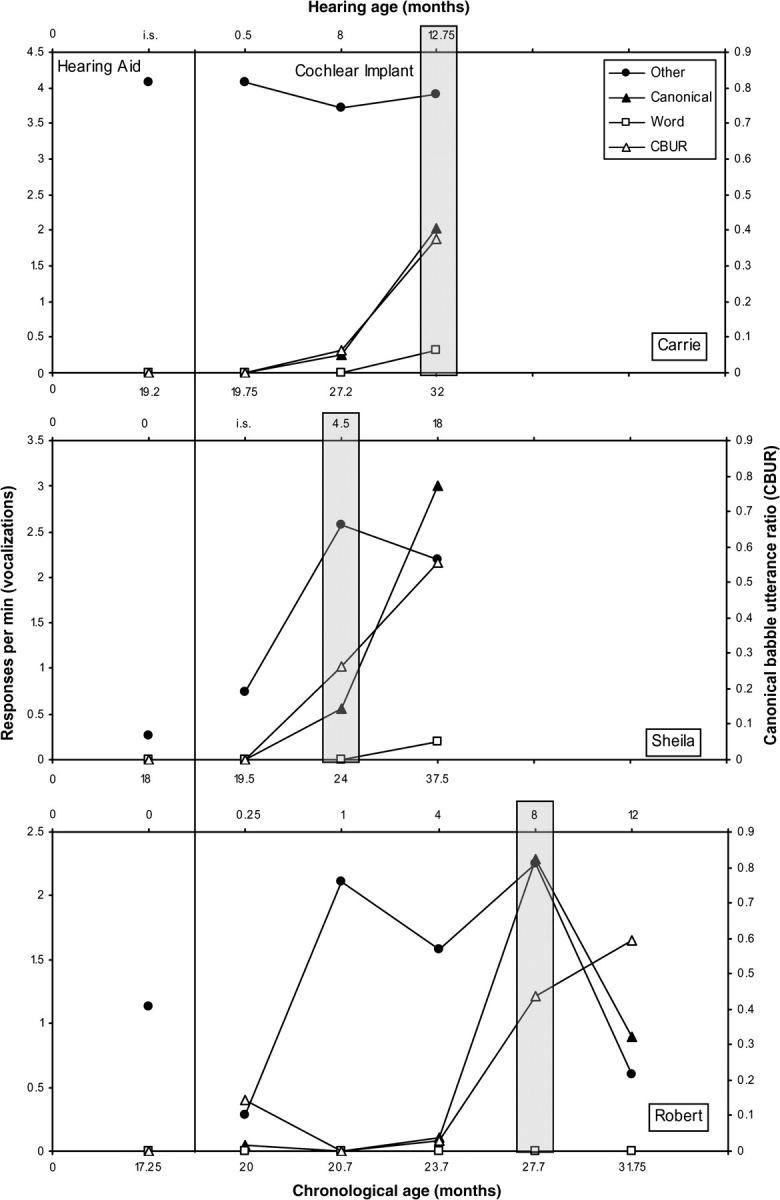
Responses per minute of vocalizations for participants with hearing loss who failed to meet criterion for audibility during hearing aid (HA) use (with Speech Intelligibility Index ≤ .31), Carrie (top), Sheila (center), and Robert (bottom). The lower x-axis represents the child's chronological age in months, and the upper x-axis represents the child's hearing age in months. I.S. indicates the day of initial stimulation of the cochlear implant (CI). An i.s. within the HA phase indicates that the vocalization sample was obtained on the day of initial stimulation but prior to initial stimulation. An i.s. within the CI phase indicates that the vocalization sample was obtained on the day of initial stimulation following initial stimulation. The absence of an i.s. indicates that no vocalization sample was obtained on the day of initial stimulation. The left y-axis represents the child's responses per minute of each of the three vocalization types as a function of age. The right y-axis represents the child's canonical babble utterance ratio (CBUR). The shaded vertical bar indicates the age of emergence of canonical babble at a criterion canonical syllable ratio and CBUR ≥ 0.15.
Figure 6.
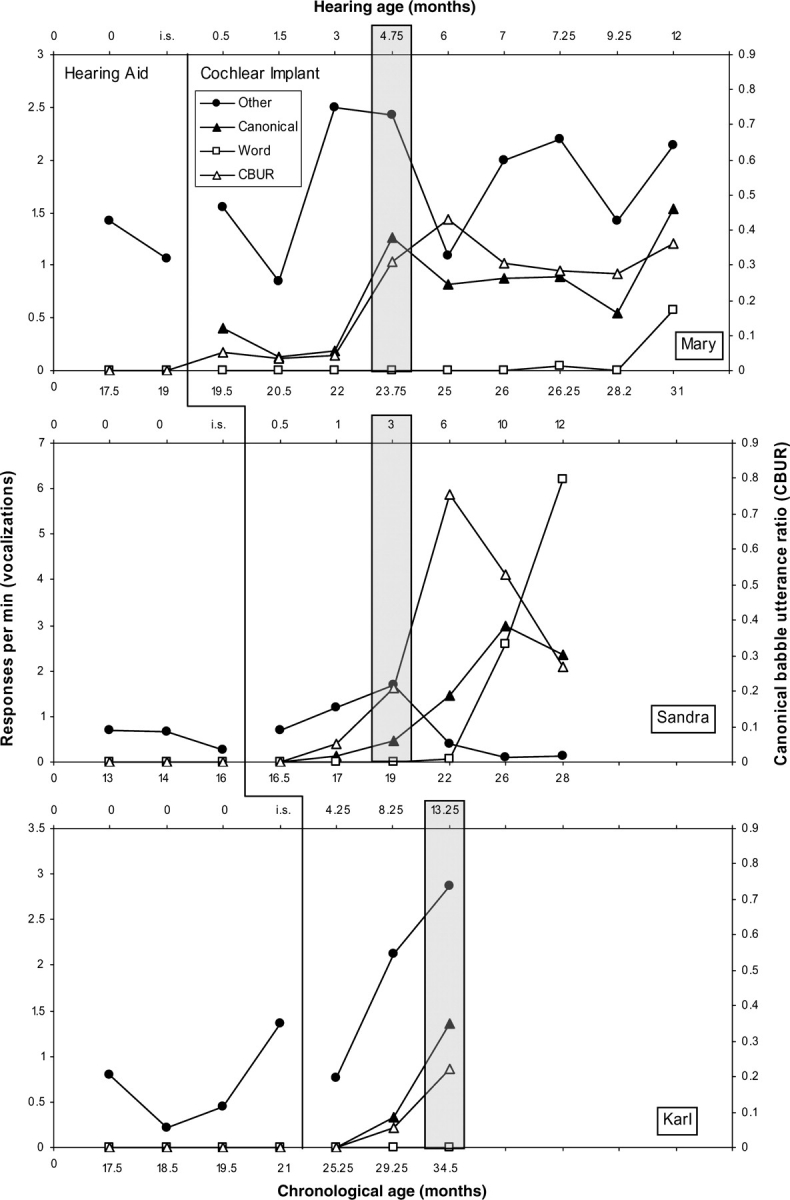
Responses per minute of vocalizations for participants with hearing loss who failed to meet criterion for audibility during hearing aid (HA) use (with Speech Intelligibility Index ≤ .31), Mary (top), Sandra (center), and Karl (bottom). The lower x-axis represents the child's chronological age in months, and the upper x-axis represents the child's hearing age in months. I.S. indicates the day of initial stimulation of the cochlear implant. An i.s. within the HA phase indicates that the vocalization sample was obtained on the day of initial stimulation but prior to initial stimulation. The left y-axis represents the child's responses per minute of each of the three vocalization types as a function of age. The right y-axis represents the child's canonical babble utterance ratio (CBUR). The shaded vertical bar indicates the age of emergence of canonical babble at a criterion canonical syllable ratio and CBUR ≥ 0.15.
Figure 7.

Responses per minute of vocalizations for participants with hearing loss who failed to meet criterion for audibility during hearing aid (HA) use (with Speech Intelligibility Index ≤ .31), Ben (top) and Kyra (bottom). The lower x-axis represents the child's chronological age in months, and the upper x-axis represents the child's hearing age in months. I.S. indicates the day of initial stimulation of the cochlear implant. An i.s. within the HA phase indicates that the vocalization sample was obtained on the day of initial stimulation but prior to initial stimulation. The left y-axis represents the child's responses per minute of each of the three vocalization types as a function of age. The right y-axis represents the child's canonical babble utterance ratio (CBUR). The shaded vertical bar indicates the age of emergence of canonical babble at a criterion canonical syllable ratio and CBUR ≥ 0.15.
Individual data: children with normal hearing.
Figure 8 shows the results of the two children with normal hearing. Data from these normal hearing children were included in the current study to illustrate that the data collection and analysis procedures were able to capture the emergence of canonical babble in the time frame indicated in the literature for children with normal hearing.
Figure 8.

Responses per minute of vocalizations for the participants with normal hearing, Mark (top) and Larry (bottom). The lower x-axis represents the child's chronological age in months, and the upper x-axis represents the child's hearing age in months. The left y-axis represents the child's responses per minute of each of the three vocalization types as a function of age. The right y-axis represents the child's canonical babble utterance ratio (CBUR). The shaded vertical bar indicates the age of emergence of canonical babble at a criterion canonical syllable ratio and CBUR ≥ 0.15.
Mark's results are displayed in the top panel of Figure 8. Mark began canonical babble at 8 months hearing age. Larry's results are displayed in the bottom panel of Figure 8. Larry began canonical babble at 9 months hearing age. Occurrence of first word production was not documented for Mark or Larry during the course of this study. Finally, it should be noted that once a CBUR ≥ 0.15 was achieved, the trend for subsequent CBURs was increasing. Exceptions to this trend occurred, for both children, in sessions immediately following onset of canonical babble.
Contributors to age of onset of canonical babble.
In those children who began canonical babble during HA use (Figures 3 and 4), it was noted that four of the five had at least 3.5 months of HA use prior to the onset of canonical babble and all had SIIs of at least .35. A multiple linear regression analysis was run to examine the contributions of these two independent variables (SII and length of HA use) to the outcome measure (age of onset of canonical babble). Two children were not included in this analysis because detailed HA information was unavailable. Children with normal hearing were included in this analysis and assigned a length of HA use of “0” months. From this analysis of 13 children, the correlation coefficient was r = .743, R2 = 0.552. Thus, we can say that the model, or linear combination of SII and length of HA use, accounts for 55% of the variation in age of onset of canonical babble. Furthermore, of the two variables in the model, only SII was a statistically significant predictor of age of onset of canonical babble (beta = −29.832, p = .006). Length of HA use had little impact on the model (beta = −0.0963, p = .807,). In fact, in a model with only SII as a predictor variable, the R2 is 0.54. Thus, adding length of HA use only increases the R2 on age of onset of canonical babble by 0.01%. It should be noted that the statistical analysis was repeated with the length of HA use as “12” months for children with normal hearing, and the results did not change.
Discussion
Fifteen children (13 of whom were diagnosed with severe–profound hearing impairment) were followed longitudinally for the development of canonical babbling. In general, the study demonstrated that (a) children with greater audibility of the speech signal during HA use began canonical babble at earlier chronological ages than did children with less audibility of the speech signal during HA use; (b) only children with an SII of greater than .35 met criterion for entry into the canonical babble stage, suggesting .35 as an essential level of audibility and a defining criterion for hearing age; (c) SII was a statistically significant predictor of age of onset of canonical babble; (d) the CBUR (at a criterion of 0.15) predicted the same age of onset of canonical babble as did the CSR for 14 of the 15 participants; and (e) once hearing age is taken into account, the majority of study participants began canonical babble in the time frame typical of children with normal hearing.
Factors Contributing to the Present Findings
Determination of audibility and changes in audibility over time.
It is possible and likely that audibility changed over time during HA use and also during CI use. Insertion gain provided by HA use was a variable required for calculation of the SII. It was sometimes the case that children had poorly fitting ear molds, and therefore, the volume setting of their HAs was reduced to prevent constant feedback. Reducing volume also results in reduced insertion gain and, therefore, a lower actual SII than predicted. In addition, each participant's audibility was determined by the best aided ear's SII. It is possible that a participant's poorer aided ear may contribute to audibility in some manner. Audibility of the speech signal may also have been reduced during an episode of otitis media. Episodes of otitis media were not followed for effect on unaided behavioral threshold; however, it is acknowledged that children with otitis media may have reduced thresholds. Finally, audibility may change depending on the type of message conveyed to children during daily routines. Audibility was calculated using the 1/3 octave band importance function for standard speech with the hip spectrum. It is likely that throughout the day, a child would receive different types of speech input in a variety of relative orientations to the speaker, both of which would affect audibility. Therefore, each participant's audibility during HA use may have been higher or lower than reported due to numerous factors.
Factors that may have affected audibility during CI use involve the process of tuning the CI. In theory, once a CI is provided, a child has access to the entire speech signal, with audibility determined primarily by the sensitivity setting of the microphone (Henry, McKay, McDermott, & Clark, 2000). In practice, a child's MAP (threshold and comfort levels of the CI) evolves over time. Many visits are required during the first year of CI use in order to fine tune a child's MAP. Manipulations in electrode threshold and comfort levels are common during the first year. In addition, depending on the microphone sensitivity, the child may have more or less audibility provided. A second factor that may affect audibility is the type of signal conveyed by the CI. The CI conveys speech as an electrical signal, and the HA conveys speech as an acoustic signal. Therefore, an SII with the CI may not equal the same SII during HA use. A third factor that may affect audibility during CI use is the use of a HA in the nonimplanted ear. Several study participants continued to wear a HA in the nonimplanted ear (Cathy, Jane, Levi, and Norman). Interestingly, the participants who did so were the same participants who met criterion for canonical babble onset during HA use and were the participants with the greatest audibility during HA use (SII ≥ 0.35). For children who wore both a HA and a CI, it is possible that the audibility provided was different from that predicted solely from CI use (Ching, Psarros, Hill, & Smither, 2002). Finally, as with HA users, it is likely that throughout the day, the child may receive different types of speech inputs in a variety of relative orientations to the speaker, both of which will affect audibility. Therefore, each participant's audibility during CI use may have been higher or lower than reported due to numerous factors.
The manner in which age of onset of canonical babble was determined.
Although the results of this study support that age of onset of canonical babble decreased as audibility of the speech signal increased, actual age of onset of canonical babble was unknown for study participants with hearing impairment. Because children were evaluated approximately once every 2 months, the age of onset reported was a conservative estimate and represented the oldest possible age of onset of canonical babble for each participant (i.e., canonical babble onset could have occurred at any point between the last visit during which canonical babble was not apparent and the first visit during which canonical babble was apparent).
Age of identification of hearing loss and subsequent HA fitting.
Age of identification of hearing loss was an additional factor that potentially affected the outcome of this study. This variable determines when the HA fitting takes place and when early intervention services begin. Hearing losses experienced by the participants of this study were identified between 3 and 15 months of age.
Age of early intervention as well as frequency and intensity of intervention.
A final factor that may have affected the outcome of this study was the amount of early intervention provided to the participants. It was routinely noticed that following cochlear implantation, children received more frequent and more intensive early intervention services. Furthermore, it was not uncommon for a child to shift from having an early interventionist visit the home once per month during HA use to receiving in home therapy weekly during CI use. The amount and intensity of early intervention services varied across participants during HA and CI use. Although no formal evaluation of early intervention services was conducted, they clearly differed among participants and potentially contributed to the study findings. Early identification of hearing loss and subsequent early intervention have been shown to be major predictors of future speech and language development (Moeller, 2000; Yoshinaga-Itano, Sedey, Coulter, & Mehl, 1998). Therefore, it is likely that age of identification and early intervention did play a role in the outcome of this study.
Limitations.
There are at least four limitations to this article. First, the children with hearing loss who participated in the study were all diagnosed with severe–profound, sensorineural hearing impairment and had no apparent cognitive or motor disabilities. Thus, applicability of the present results to other degrees and types of hearing impairment and to children with cognitive and motor disabilities is limited. Specifically, for some children with motor “speech” impairments, canonical babbling may not be an accurate indicator of benefit from HA use (Kishon-Rabin et al., 2005). It is safe to infer, however, that children with hearing impairment that is not as severe would benefit similarly from strategies that maximize audibility. Second, age of enrollment prevented a detailed within-participant comparison of vocal development between the HA and CI phases. That is, children who were enrolled at older ages had fewer vocalization samples prior to receiving a CI. One potential benefit of the range of age of enrollment is that it provided varying lengths of time spent within the HA phase and the CI phase and thus showed that criterion for audibility and not chronological age accounted for vocal development. This effect is demonstrated by the single subject graphs displayed in a nonconcurrent multiple baseline format. Third, the number of sessions conducted during the HA and CI phases for some participants can be seen as a limitation. Specifically, for four participants, too few data points were obtained during the HA phase to determine a trend in the data. However, taken collectively, the direction in the overall rate of vocalizations was similar across all participants. Finally, the session length (number of minutes of data collection for any given session) varied per visit and across participants as described in the Method section. This variation could account for a systematic difference in the results, in that longer sessions might result in greater CBURs or vice versa. To investigate this issue, a Pearson Product Moment Correlation was calculated using the number of minutes of each session and the CBUR calculated for that session. The resulting correlation showed no significant relationship with a small correlation coefficient of .168.
Clinical Implications
Given the demonstration of the relationship between audibility during HA use and canonical babbling, the current study highlights the importance of obtaining complete behavioral evaluations to establish accurate thresholds for use in the HA fitting for children with all degrees of hearing impairment. For young children with newly identified hearing impairment, threshold information must initially be taken from physiological test measures (e.g., auditory brainstem response and auditory steady-state response). Although these measures do provide reasonable estimates of hearing sensitivity, there is not a one-to-one correspondence between these physiological measures and behavioral thresholds (Gorga et al., 1985; Johnson & Brown, 2005; Stapells, Gravel, & Martin, 1995; Vander Werff & Brown, 2005). Therefore, clinicians involved in the management of children with hearing impairment should make it a priority to obtain a complete behavioral audiological evaluation to optimize the fitting of amplification.
The current study also highlights the importance of pediatric audiologists following current guidelines regarding the use of probe microphone measures and calculation of audibility (e.g., SII) during the HA fitting (American Academy of Audiology, 2004; Ministry of Children and Youth Services, 2007; The Pediatric Working Group, 1996). These guidelines allow for the necessary integration of physiological and behavioral measures to maximize audibility when working with young children. Procedures to quantify audibility are well defined, readily available, and automatically calculated in new technology used for the fitting of HAs (e.g., Audioscan Verifit Hearing Aid Analyzer System) as well as in computer programs specifically designed for the calculation of audibility.
Managing hearing loss in this manner could benefit children with severe–profound hearing impairment. Likewise, HA use preimplant (when audibility is maximized) may accelerate postimplant vocal development. Children with SIIs of .35 or greater during HA use began first oral-word production, on average, 3.4 months earlier than did children with SIIs less than .35 during HA use.
Methodological Contributions
In addition to clinical implications, this study also contributes to the existing literature on vocal development. First, this study adds to the methods used to classify a child's vocalizations as canonical. Specifically, in much of the previous child vocalization research, canonical babble has been determined through the time-consuming and labor-intensive process of individual syllable counting. In place of an analysis in which each vocalization coded as canonical is individually analyzed for the number of syllables present (as is the case with CSR), the CBUR can be calculated from the data generated from a computerized coding program such as that used in this study. This method can save time in the analysis phase and demonstrates promise as a quick method to determine, at least perceptually, when a child has likely entered the canonical babbling phase. This study demonstrates support for the use of this more efficient method (CBUR) as age of onset of canonical babble determined by the CBUR agreed with that determined by the CSR for 14 of the 15 participants at the same criterion of 0.15. For the one participant (Axel) whose age of onset differed when determined using the CBUR (8.6 months) and CSR (3.5 months) methods, the CBUR was always less than the CSR and therefore potentially represents a more conservative estimate of age of onset of canonical babble. Because of the propensity of the CBUR to be a conservative measure (giving credit for babble at the utterance vs. the syllable level), it may be that the criterion for entry into the canonical babble stage with the CBUR should be less than that with the CSR. In the case of Axel (Figure 3), his CBUR at 3.5 months of age was 0.14. Furthermore, the conservative nature of the CBUR may allow it to serve as a predictor of when canonical productions have become more stable or abundant. As indicated in the results for participants with hearing impairment, once a CBUR of 0.15 was achieved, subsequent CBURs generally did not fall below this value.
Second, this study expands the current literature by relating the audibility a child receives through the use of an amplification device to the child's vocal development. The calculation of the SII in combination with the methods described above to identify onset of canonical babble may explain discrepancies between the current study's findings and those previously reported in the literature. For example, this article demonstrates that some children with more severe hearing impairment receive enough audibility from HAs to enter the canonical babbling stage in a manner similar to children with normal hearing. This finding is in contrast to the previous literature for children with more severe losses (e.g., Stoel-Gammon & Otomo, 1986).
Finally, this article supports the consideration of hearing age (as defined in the Trends in Vocal Development section) in documenting the onset of canonical babble. Once hearing age was taken into account, the majority of children with hearing impairment (10 of the 13) began canonical babble by 9 months hearing age. In general, these individual results agree and expand upon the results found in the case studies of Kent et al. (1987) and Oller et al. (1985). It should be noted that the remaining children with hearing impairment (Carrie, Karl, and Kyra) who began canonical babble at later hearing ages had gaps in data collection around the time that onset may occur in children with normal hearing. Therefore, onset of canonical babble within the time frame typical of children with normal hearing cannot be completely ruled out.
Future Directions
This article highlights the need for future research in the area of audibility and infant vocal development. Specifically, there is a need to explore the relationship between onset and complexity of canonical babble and later vocalization development for children with all degrees of hearing impairment when audibility is well documented. For children with severe–profound hearing impairment, what is the predictability of onset and complexity of canonical babble to future speech and language development? Preliminary results from Walker and Bass-Ringdahl (2007) suggest that the complexity of a child's vocalizations at 6–9 months post-CI predicts future speech and language development at 48 months chronological age. Furthermore, the prognostic indications of early infant vocalizations may help clinicians identify the need to increase services and/or make changes to a child's amplification/intervention plan.
A second area in need of investigation is the impact of changes in audibility over time on infant vocal development. This article clearly indicated a positive relationship between infant vocal development and degree of audibility; therefore, it is important to investigate variables known to contribute to audibility. For example, what impact do factors such as a loose-fitting earmold, an ear infection, and lack of consistent HA use have on audibility and subsequent vocal development? The concept of essential audibility should be more thoroughly explored. In this article, children did not begin canonical babble until achieving an SII of at least .35. Does this relationship hold with larger numbers of children and across all degrees of hearing impairment?
A third area for future discussion concerns the use of the terms “hearing age” and “listening experience.” As indicated in the statistical analysis, albeit limited by number of study participants, length of HA use (or listening experience) was not a significant predictor of age of onset of canonical babble. This result may be misinterpreted to mean that time logged with a HA is inadequate to signal the beginning of a child's hearing age for vocalization development. On the contrary, the results of the current study imply that listening experience is important when considered in conjunction with degree of audibility. Upon examination of this study's individual participant data (Figures 3–7), this discrimination can be more clearly discerned. That is, once hearing age (as defined in this study) was taken into account, study participants began canonical babble in the time frame typical of children with normal hearing. Because of the weight such terms as hearing age and listening experience carry in clinical and medical decision making, their use needs to be carefully considered. Should hearing age be defined in a manner more consistent with that used in this article? That is, hearing age only begins after an “essential” level of audibility is achieved. Does a different term need to be adopted to indicate listening experience post-HA fitting? A term that gives credit to listening achieved via the HA fitting that might not lead to the onset of canonical babble. Additional investigation with larger numbers of children may help to clarify these relationships and terms.
Last, but perhaps most important, what is the contribution of “stepped up” early intervention to improved vocal development postimplant? The literature clearly indicates the importance of early consistent intervention, yet this is one of the most difficult areas to quantify and compare in studies such as the current investigation.
More definitive answers to the questions posed above have the potential to streamline the decision-making process for families and for professionals. In a time when the age of cochlear implantation is rapidly declining and approaching 6 months of age, difficult decisions regarding intervention are being made without relevant research serving as a guide. Infant vocalization development and audibility need to be defined in clinically useable ways to meaningfully contribute to the decision-making process.
Funding
This research is based on the author's doctoral dissertation submitted to The University of Iowa and was supported in part by research grant 2 P50 DC00242 from the National Institutes on Deafness and Other Communication Disorders, National Institutes of Health; grant RR00059 from the General Clinical Research Centers Program, Division of Research Resources, National Institutes of Health; the Lions Clubs International Foundation; and the Iowa Lions Foundation.
Conflict of Interest
No conflicts of interest were reported.
Acknowledgments
Portions of this article were presented at the 6th International Cochlear Implant Conference, Miami, FL, 2000; the 8th Symposium Children’s Cochlear Implant Conference, Los Angeles, CA, 2001; the American Speech-Language Hearing Association Conference, 2002; the American Academy of Audiology Conference, 2002; and the 7th International Cochlear Implant Conference, Manchester, England, 2002. The author thanks Bruce Tomblin, Lenore Holte, David Wacker, Jerald Moon, Carolyn Brown, and Jan Moore for their mentorship during the completion of this project; Joel Ringdahl, Mary Pat Moeller, Brittan Barker, and Christopher Turner for their helpful comments during editing and Jacob Oleson for his statistical consultations; Robin Criter and Ashley Burke for their tireless assistance in data analysis as well as D. Kimbrough Oller for personal communications related to data analysis; and the infants and their families who have volunteered so much of their time to The University of Iowa Children’s Cochlear Implant Program.
Appendix A: First Pass of Coding to Identify Vocalization Type at the Level of the Breath Group
Definitions
Canonical (C): Code as canonical any utterance that contains a minimum of one consonant and one vowel (e.g., [ba], [ama], [bababa], [gagaba]).
Liquids and glides should be counted as consonants (e.g., [ja], [lai], [wa]).
[h] and glottal stops should not be counted as consonants (e.g., [uh], [uhuh], [ha], [ah]).
Word (W): A recognizable word.
Other (O): Code as an other(s) typical vocal play sounds, such as squeals and growls (pitch changes), yells and whispers (loudness changes), trills, raspberries, snorts, friction noises, consonant-like sounds, vowel-like sounds, vowels (fully resonant nuclei), and nasalized vowels (quasi-resonant nuclei—a vowel produced without a fully open vocal tract).
Those utterances that follow the consonant–vowel form but are judged auditorily as not meeting the percept of being well formed and adult like should be placed in this category. These utterances are considered Marginal. The transition between consonant and vowel may be audible in these utterances.
Exclusions: Do not code sighs, grunts, breathing noises, laughing, crying, or other bodily function noises, such as coughing, sneezing, burping, yawning or hiccupping.
Rules for Coding
Coding occurs by breath group. A breath group is defined as a vocalization or grouping of vocalizations demarcated by a period of quiet of at least 2 s. After a vocalization has ended, count 1-1000, 2-1000 to demarcate breath groups. If the child begins vocalizing again before 2-1000 is completed, it is the same breath group.
Code each vocalization type once per breath group (e.g., [baba…mama…dada] = 1 Canonical).
If vocalization type changes within a breath group, code the new vocalization type (e.g., [a…bababa] = 1 Other and 1 Canonical).
If vocalization type switches to a previously coded vocalization type within the same breath group, do not code the vocalization type a second time (e.g., [a…baba…a] = 1 Other and 1 Canonical).
Each word is coded even if it occurs in the same breath group (e.g., [I want that] = 3 Words).
Code each vocalization type as soon as possible to ensure accuracy while maintaining the rules listed above regarding breath groups.
Appendix B: Second Pass of Coding to Conduct Syllable Count
The purpose for conducting a syllable count is to calculate the Canonical Syllable Ratio or CSR (the number of canonical syllables divided by the total number of syllables).
In order to calculate a CSR for a session under review, at least one utterance must be coded as Canonical during the first pass of coding (all 10-min blocks included).
- If the above criterion is met, transcribe and count the number of canonical syllables (consonant–vowel or vowel–consonant combinations) present for each utterance coded as Canonical during the first pass of coding. Use the same inclusion and exclusion criteria as described for Canonical in Appendix A.
- (a) The number of canonical syllables determined will serve as the numerator for the calculation of the CSR for the session under evaluation.
- (b) When evaluating utterances, if you determine that a canonical syllable is not present, it will not be included in the numerator for calculation of the CSR. However, if the vocalization meets the criteria outlined below (in 4b–4e) it will be included in the denominator.
After transcribing and counting canonical syllables, count utterances coded as Other during the first pass of coding in the session under review.
- Syllables from (3) that will constitute the “Total Syllable” denominator for the calculation of CSR must meet the following criteria:
- (a) Canonical syllable.
- (b) Marginal syllable.
- (c) Fully resonant nuclei. This includes all vowel sounds that are produced with a fully open vocal track. Perceptually they will be “normal” sounding vowels.
- (d) Quasi-resonant nuclei. This includes all vowel sounds that are produced with some constriction in the vocal track. Perceptually these might sound “flat.”
- (e) Any vocalization that is voiced (with the exception of any vocalization that is listed as an Exclusion in Appendix A). If voicing is ambiguous, do not count.
References
- American Academy of Audiology. Pediatric amplification guideline. Audiology Today. 2004, March/April;16:46–53. [Google Scholar]
- American National Standards Institute (ANSI) ANSI S3.5-1997. American national standard methods for calculation of the speech intelligibility index. New York: Author; 1997. [Google Scholar]
- Bayley N. Bayley scales of infant development—II. San Antonio, TX: Psychological Corporation; 1993. [Google Scholar]
- Centers for Disease Control and Prevention. 2007 CDC EHDI hearing screening and follow-up survey (HSFS) 2007 Retrieved October 5, 2009, from www.cdc.gov/ncbddd/ehdi/data.htm. [Google Scholar]
- Ching TYC, Psarros C, Hill M, Smither J. Should children who wear a cochlear implant in one ear use a hearing aid in the opposite ear? In: Seewald RC, Gravel JS, editors. A sound foundation through early amplification 2001: Proceedings of the Second International Conference. Bury St Edmund, UK: St. Edmundsbury Press; 2002. pp. 195–202. [Google Scholar]
- Eilers RE, Oller DK. Infant vocalizations and the early diagnosis of severe hearing impairment. Journal of Pediatrics. 1994;124:199–203. doi: 10.1016/s0022-3476(94)70303-5. [DOI] [PubMed] [Google Scholar]
- Eilers RE, Oller DK, Levine S, Basinger D, Lynch MP, Urbano R. The role of prematurity and socioeconomic status in the onset of canonical babbling in infants. Infant Behavior and Development. 1993;16:297–315. [Google Scholar]
- Ertmer DJ, Mellon JA. Beginning to talk at 20 months: Early vocal development in a young cochlear implant recipient. Journal of Speech, Language, and Hearing Research. 2001;44:192–206. doi: 10.1044/1092-4388(2001/017). [DOI] [PubMed] [Google Scholar]
- Gorga MP, Worthington DW, Reiland JK, Beauchaine KA, Goldgar DE. Some comparisons between auditory brain stem response thresholds, latencies, and the pure-tone audiogram. Ear and Hearing. 1985;6:105–112. doi: 10.1097/00003446-198503000-00008. [DOI] [PubMed] [Google Scholar]
- Hapsburg D, Davis BL. Auditory sensitivity and the prelinguistic vocalizations of early-amplified infants. Journal of Speech, Language, and Hearing Research. 2006;49:809–822. doi: 10.1044/1092-4388(2006/057). [DOI] [PubMed] [Google Scholar]
- Hedley-Williams A, Tharpe AM, Bess FH. Fitting hearing aids in the pediatric population: A survey of practice procedures. In: Bess FH, Gravel JS, Tharpe AM, editors. Amplification for children with auditory deficits. Nashville, TN: Bill Wilkerson Center Press; 1996. pp. 107–122. [Google Scholar]
- Henry BA, McKay CM, McDermott HJ, Clark GM. The relationship between speech perception and electrode discrimination in cochlear implantees. Journal of the Acoustical Society of America. 2000;108:1269–1280. doi: 10.1121/1.1287711. [DOI] [PubMed] [Google Scholar]
- Hicks CB, Tharpe AM, Ashmead DH. Behavioral auditory assessment of young infants: Methodological limitations or natural lack of auditory responsiveness. American Journal of Audiology. 2000;9:124–130. doi: 10.1044/1059-0889(2000/015). [DOI] [PubMed] [Google Scholar]
- Johnson T, Brown C. Threshold prediction using the auditory steady-state response and the tone burst auditory brain stem response: A within-subject comparison. Ear and Hearing. 2005;26:559–576. doi: 10.1097/01.aud.0000188105.75872.a3. [DOI] [PubMed] [Google Scholar]
- Kennedy CH. Single-case designs for educational research. Boston: Allyn and Bacon; 2005. [Google Scholar]
- Kent RD, Osberger MJ, Netsell R, Goldschmidt Hustedde C. Phonetic development in identical twins differing in auditory function. Journal of Speech and Hearing Disorders. 1987;52:64–75. doi: 10.1044/jshd.5201.64. [DOI] [PubMed] [Google Scholar]
- Kishon-Rabin L, Taitelbaum-Swead R, Ezrati-Vinacour R, Hildesheimer M. Prelexical vocalizations in normal hearing and hearing-impaired infants before and after cochlear implantation and its relation to early auditory skills. Ear and Hearing. 2005;26:17S–29S. doi: 10.1097/00003446-200508001-00004. [DOI] [PubMed] [Google Scholar]
- Kruger B. An update on the external resonance in infants and young children. Ear and Hearing. 1987;8:333–336. doi: 10.1097/00003446-198712000-00008. [DOI] [PubMed] [Google Scholar]
- Lynch MP, Oller DK, Steffens ML, Levine SL, Basinger DL, Umbel V. Onset of speech-like vocalizations in infants with Down Syndrome. American Journal on Mental Retardation. 1995;100:68–86. [PubMed] [Google Scholar]
- Ministry of Children and Youth Services. Ministry of Children and Youth Services, Ontario, Canada: Ontario infant hearing program protocol for the provision of amplification, version 3.1. 2007 Retrieved December 28, 2009, from www.mountsinai.on.ca/care/infant-hearingprogram/documents/amplification_revision_2007_006.pdf. [Google Scholar]
- Moeller MP. Early intervention and language development in children who are deaf and hard of hearing. Pediatrics. 2000;106:1–9. doi: 10.1542/peds.106.3.e43. [DOI] [PubMed] [Google Scholar]
- Moeller MP, Hoover B, Putman C, Arbataitis K, Bohnenkamp G, Peterson B, et al. Vocalizations of infants with hearing loss compared with infants with normal hearing: Part I—phonetic development. Ear and Hearing. 2007;28:605–627. doi: 10.1097/AUD.0b013e31812564ab. [DOI] [PubMed] [Google Scholar]
- Moodie KS, Seewald RC, Sinclair ST. Procedures for predicting real-ear hearing aid performance in young children. American Journal of Audiology. 1994;3:23–31. [Google Scholar]
- National Institutes of Health Consensus Statement. Early identification of hearing impairment in infants and young children. 1993 Retrieved December 31, 2009, from http://consensus.nih.gov/1993/1993HearingInfantsChildren092html.htm. [PubMed] [Google Scholar]
- Nikolopoulos TP, Archbold SM, Gregory S. Young deaf children with hearing aids or cochlear implants: Early assessment package for monitoring progress. International Journal of Pediatric Otorhinolaryngology. 2005;69:175–186. doi: 10.1016/j.ijporl.2004.08.016. [DOI] [PubMed] [Google Scholar]
- Oller DK. The emergence of the sounds of speech in infancy. In: Yeni-Komshaian GH, Kavanagh JF, Ferguson CA, editors. Child phonology: Volume 1. Production. New York: Academic Press; 1980. pp. 93–110. [Google Scholar]
- Oller DK. The emergence of the speech capacity. Mahwah, NJ: Lawrence Erlbaum; 2000. [Google Scholar]
- Oller DK, Eilers RE. The role of audition in infant babbling. Child Development. 1988;59:441–449. [PubMed] [Google Scholar]
- Oller DK, Eilers RE, Basinger D. Intuitive identification of infant vocal sounds by parents. Developmental Science. 2001;4:49–60. [Google Scholar]
- Oller DK, Eilers RE, Bull DH, Carney AE. Prespeech vocalizations of a deaf infant: A comparison with normal metaphonological development. Journal of Speech and Hearing Research. 1985;28:47–63. doi: 10.1044/jshr.2801.47. [DOI] [PubMed] [Google Scholar]
- Oller DK, Lynch MP. Infant vocalizations and innovations in infraphonology: Toward a broader theory of development and disorders. In: Ferguson C, Menn L, Stoel-Gammon C, editors. Phonological development. Parkton, MD: York Press; 1992. pp. 509–536. [Google Scholar]
- The Pediatric Working Group. Amplification for infants and children with hearing loss. American Journal of Audiology. 1996;5:53–68. [Google Scholar]
- Pinto E, Lacerda C, Porto P. Comparison between the IT-MAIS and MUSS questionnaires with video-recording for evaluation of children who may receive a cochlear implantation. Brazilian Journal of Otorhinolaryngology. 2008;74:91–98. doi: 10.1016/S1808-8694(15)30757-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rigsby KM, Bradham TS, Dickinson W, Mueller HG. Current practices in pediatric audiology. Division 9 Newsletter, ASHA. 2007;17:3–7. [Google Scholar]
- Robbins AM, Koch DB, Osberger MJ, Zimmerman-Phillips S, Kishon-Rabin L. Effect of age at implantation on auditory-skill development in infants and toddlers. Archives of Otolaryngology Head and Neck Surgery. 2004;130:570–574. doi: 10.1001/archotol.130.5.570. [DOI] [PubMed] [Google Scholar]
- Rvachew S, Slawinski EB, Williams M, Green CL. The impact of early onset otitis media on babbling and early language development. Journal of the Acoustical Society of America. 1999;105:467–475. doi: 10.1121/1.424575. [DOI] [PubMed] [Google Scholar]
- Sander M. !Observe: A behavior recording and reporting software program [Computer software and manual] Longmont, CO: Sopris West; 2001. [Google Scholar]
- Seewald RC. The desired sensation level (DSL) method for hearing aid fitting in infants and children. Phonak Focus. 1995;20 Stafa, Switzerland: Phonak AG. [Google Scholar]
- Seewald RC, Hudson SP, Gagne JP, Zelisko DL. Comparison of two procedures for estimating the sensation level of amplified speech. Ear and Hearing. 1992;13:142–149. doi: 10.1097/00003446-199206000-00002. [DOI] [PubMed] [Google Scholar]
- Seewald RC, Mills J, Bagatto M, Scollie S, Moodie S. A comparison of manufacturer-specific prescriptive procedures for infants. Hearing Journal. 2008;61:26–34. [Google Scholar]
- Seewald RC, Scollie SD. An approach for ensuring accuracy in pediatric hearing instrument fitting. Trends in Amplification. 2003;7:29–40. doi: 10.1177/108471380300700104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith BL, Oller DK. A comparative study of pre-meaningful vocalizations produced by normally developing and Down’s syndrome infants. Journal of Speech and Hearing Disorders. 1981;46:46–51. doi: 10.1044/jshd.4601.46. [DOI] [PubMed] [Google Scholar]
- Stapells DR, Gravel JS, Martin BA. Thresholds for auditory brainstem responses to tones in notched noise from infants and young children with normal hearing or sensorineural hearing loss. Ear and Hearing. 1995;16:361–371. doi: 10.1097/00003446-199508000-00003. [DOI] [PubMed] [Google Scholar]
- Stark RE. Stages of speech development in the first year of life. In: Yeni-Komshaian GH, Kavanagh JF, Ferguson CA, editors. Child phonology: Volume 1. Production. New York: Academic Press; 1980. pp. 73–90. [Google Scholar]
- Steffens ML, Oller DK, Lynch M, Urbano RC. Vocal development in infants with Down syndrome and infants who are developing normally. American Journal on Mental Retardation. 1992;97:235–246. [PubMed] [Google Scholar]
- Stelmachowicz P, Hoover B. Hearing instrument fitting and verification for children. In: Katz J, Medwetsky L, Burkard R, Hood L, editors. Handbook of clinical audiology, sixth edition. Baltimore: Lippincott Williams & Wilkins; 2009. pp. 827–845. [Google Scholar]
- Stelmachowicz P, Lewis D, Kalberer A, Creutz T. Situational hearing-aid response profile (SHARP), Version 2.0: User's manual. Omaha, NE: Boys Town National Research Hospital; 1994. [Google Scholar]
- Stoel-Gammon C, Otomo K. Babbling development of hearing-impaired and normally hearing subjects. Journal of Speech and Hearing Disorders. 1986;51:33–41. doi: 10.1044/jshd.5101.33. [DOI] [PubMed] [Google Scholar]
- Vander Werff K, Brown C. Effect of audiometric configuration on threshold and suprathreshold auditory steady-state responses. Ear and Hearing. 2005;26:310–326. doi: 10.1097/00003446-200506000-00007. [DOI] [PubMed] [Google Scholar]
- Vohr BR, Carty LM, Moore PE, Letourneau K. The Rhode Island hearing assessment program: experience with statewide hearing screening (1993-1996) Journal of Pediatrics. 1998;133:353–357. doi: 10.1016/s0022-3476(98)70268-9. [DOI] [PubMed] [Google Scholar]
- Walker EA, Bass-Ringdahl S. Babbling complexity and its relationship to speech and language outcomes in children with cochlear implants. Otology and Neurotology. 2007;29:225–229. doi: 10.1097/mao.0b013e31815f6673. [DOI] [PubMed] [Google Scholar]
- Yoshinaga-Itano C, Sedey A, Coulter DK, Mehl AL. Language of early and later identified children with hearing loss. Pediatrics. 1998;102:1161–1171. doi: 10.1542/peds.102.5.1161. [DOI] [PubMed] [Google Scholar]